Hepatitis Delta Virus Coinfection Triples Liver Cancer Risk in Hepatitis B Patients
November 5, 2024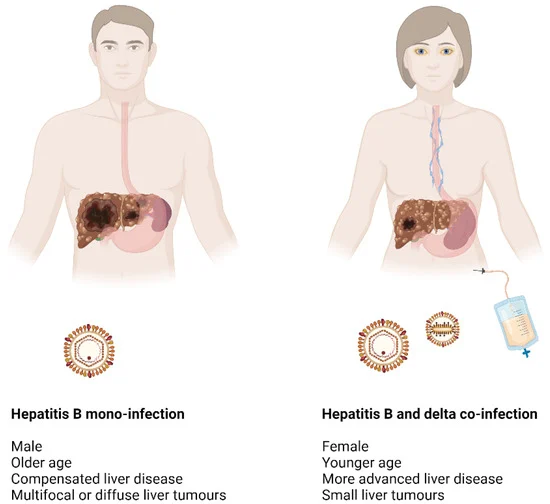
While HDV increases the risk of HCC associated with HBV, the precise mechanisms behind its carcinogenic potential remain unclear.
Molecular mechanisms of HDV infection involve its recognition by pattern recognition receptors (PRRs), which trigger an immune response mediated by interferons.
In cases of HBV/HDV co-infection, a robust innate immune response is activated, characterized by the recruitment of immune cells and the activation of interferon-stimulated genes.
Although innate immune responses are crucial for controlling HBV and HDV infections, they can also lead to liver damage due to the inflammatory response.
Recent studies highlight the role of specific immune cell types, such as natural killer (NK) cells and T cells, in the liver's response to HBV and HDV infections, underscoring the complexity of these immune interactions.
The relationship between HBV and HDV is intricate, with HDV potentially exerting both direct and indirect oncogenic effects, including alterations in the tumor microenvironment and immune response.
Chronic hepatitis B virus (HBV) infection affects approximately 250-300 million individuals worldwide, with a significant portion developing chronic conditions that can lead to liver cirrhosis and hepatocellular carcinoma (HCC).
Hepatitis B virus and hepatitis delta virus (HDV) coinfection accounts for 8-10% of HCC cases globally, with epidemiological studies indicating that this coinfection occurs in 4.5-13% of individuals infected with HBV.
Research shows that HDV can significantly exacerbate liver damage in HBV-infected patients, tripling the likelihood of developing HCC and doubling hepatitis-related mortality rates.
Patients with chronic HBV-HD coinfection face a higher incidence of liver cirrhosis and HCC compared to those with HBV alone, with a median progression time of five years to cirrhosis and ten years to HCC.
Active replication of HDV is a notable risk factor for HCC development, presenting a three-fold increase in long-term risk, although this risk diminishes once cirrhosis is established.
The clinical management of HCC in patients with HBV-HD coinfection presents unique challenges due to the complex interplay between the two viruses and the severity of liver disease.
Summary based on 2 sources